Metabolism
on-line - the virtual tutorial room
copyright © 2008 - 2015 David A Bender
An unconscious child with keto-acidosis and a skin rash

 Barry
is the second child of parents who are first cousins; his brother is 5 years
old, fit and healthy. He was born at full term after an uneventful pregnancy,
weighing 3.4 kg (the 50th centile), and developed normally until he was 6 months
old, after when he showed some retardation of development. He also developed
a fine scaly skin rash about this time, and his hair, which had been normal,
became thin and sparse.
Barry
is the second child of parents who are first cousins; his brother is 5 years
old, fit and healthy. He was born at full term after an uneventful pregnancy,
weighing 3.4 kg (the 50th centile), and developed normally until he was 6 months
old, after when he showed some retardation of development. He also developed
a fine scaly skin rash about this time, and his hair, which had been normal,
became thin and sparse.
At 9 months of age he was admitted to UCL Hospital in a coma; emergency clinical
chemistry results on a plasma sample were as follows:
Barry |
Reference range |
|
| pH | 6.9 |
7.35 - 7.45 |
| Bicarbonate, mmol /L | 2.0 |
21 - 25 |
| Ketone bodies, mmol /L | 21 |
1 - 2.5 |
| Lactate, mmol /L | 7.3 |
0.5 - 2.2 |
| Pyruvate, mmol /L | 0.31 |
< 0.15 |
| Glucose, mmol /L | 3.3 |
3.5 - 5.5 |
What treatment should he be given in the Emergency Room?
His immediate problem is severe acidosis, so the most appropriate emergency treatment would be intravenous infusion of bicarbonate to permit respiratory compensation for the acidosis by exhaling carbon dioxide, so shifting the bicarbonate equilibrium to the right:.
![]()
He regained consciousness rapidly. Over the next few days he continued to respire rapidly, and even after a meal he excreted ketone bodies in his urine. His plasma glucose remained in the low normal range, and his plasma insulin was normal both in the fasting state and in response to an oral load of 50g of glucose /kg body weight.
Why do you think he was respiring rapidly?
Rapid respiration is a response to acidosis - an attempt to breathe out carbon dioxide and so shift the equilibrium above to the right, and raise plasma pH.
The fact that he was excreting ketone bodies suggests that he was still suffering from keto-acidosis. Without further information it is difficult to account for ketosis in the fed state after a meal.
Do you think that a likely diagnosis would be diabetes mellitus?
The normal fasting plasma insulin and the normal response to a glucose load means that we can rule out diabetes mellitus.
 Analysis
of his urine by high pressure liquid chromatography revealed that he was excreting
relatively large amounts of a variety of organic acids that are not normally
excreted.
Analysis
of his urine by high pressure liquid chromatography revealed that he was excreting
relatively large amounts of a variety of organic acids that are not normally
excreted.
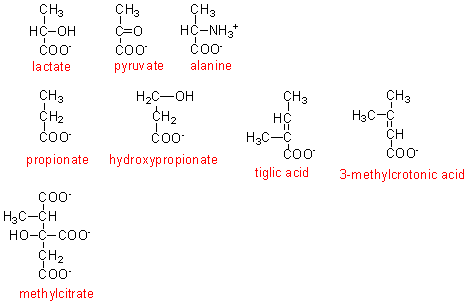
In addition to the compounds shown on the right, he was also excreting glycine conjugates of propionic, tiglic and methylcrotonic acids.
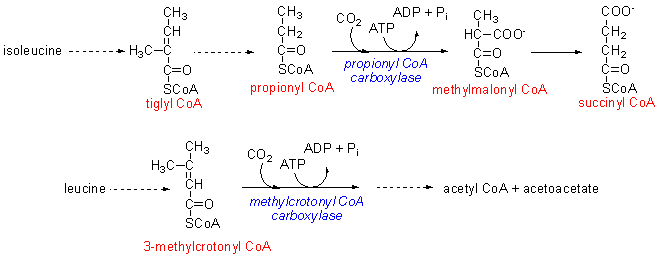
As shown below, tiglyl CoA is an intermediate in the metabolism of isoleucine, and normally is metabolised onwards, via propionyl CoA to yield succinyl COA, an intermediate of the citric acid cycle.
3-Methylcrotonyl CoA is an intermediate in the metabolism of isoleucine, and is normally metabolised onwards to acetyl CoA and acetoacetate.
What is the most likely reason to explain why he is excreting tiglic, propionic and 3-methylglutaric acids and their glycine conjugates in his urine?
If he cannot metabolise tiglyl CoA, propionyl CoA and 3-methylcrotonyl CoA onwards for some reason, then as these accumulate, they will be hydrolysed to salvage the CoA, leaving the free acids. These cannot be metabolised further, and will be excreted in the urine.
Many organic acids are conjugated with glycine (and sometimes also alanine) before excretion. Excessive intake of e.g. benzoic acid can outstrip the body's capacity for glycine synthesis, so impairing protein synthesis and rendering glycine a partially essential amino acid
What is the likely source of the methylcitrate he is excreting?
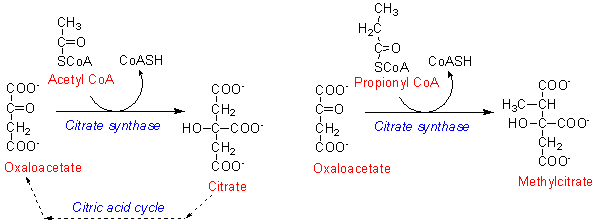 As shown
on the right, propionyl CoA is an alternative substrate for citrate synthase,
forming methylcitrate. Methylcitrate cannot be metabolised further, and so is
excreted in the urine.
As shown
on the right, propionyl CoA is an alternative substrate for citrate synthase,
forming methylcitrate. Methylcitrate cannot be metabolised further, and so is
excreted in the urine.
What is the metabolic outcome of forming methylcitrate from propionyl CoA and oxaloacetate?
There will be depletion of oxaloacetate, leading to a reduction of citric acid cycle activity, and hence a deficit in ATP formation.
What will be the metabolic outcome of reduced ATP formation due to reduced citric acid cycle activity?
As ADP accumulates, it undergoes reaction to form 5'AMP and ATP, catalysed
by adenylate kinase. ![]()
This is a very minor source of ATP, but the 5'AMP acts as a metabolic signal; among other actions it results in increased beta-oxidation of fatty acids in the liver, for ATP formation.
Can you account for Barry's continued formation of ketone bodies and ketonuria, even in the fed state?
5'AMP leads to increased beta-oxidation of fatty acids in the liver. However, because of the lack of oxaloacetate, the acetyl CoA arising from beta-oxidation cannot be metabolised through the citric acid cycle, and can only be used for synthesis of ketone bodies.