Metabolism
on-line - the virtual tutorial room
copyright © 2008 - 2015 David A Bender
Gripping abdominal pain and jaundice
 GS
is a 40 year old, slightly overweight, woman. Recently she has suffered episodes
of what she described as "gripping abdominal pain" after meals, and
she had noticed that her faeces were paler than usual, and floated in the lavatory
pan, but her urine was darker than usual.
GS
is a 40 year old, slightly overweight, woman. Recently she has suffered episodes
of what she described as "gripping abdominal pain" after meals, and
she had noticed that her faeces were paler than usual, and floated in the lavatory
pan, but her urine was darker than usual.
When she visited her GP he noted that she had a sallow complexion, and the whites of her eyes were yellow.
What might account for her jaundice?
Why do you think her faeces were pale and her urine dark?
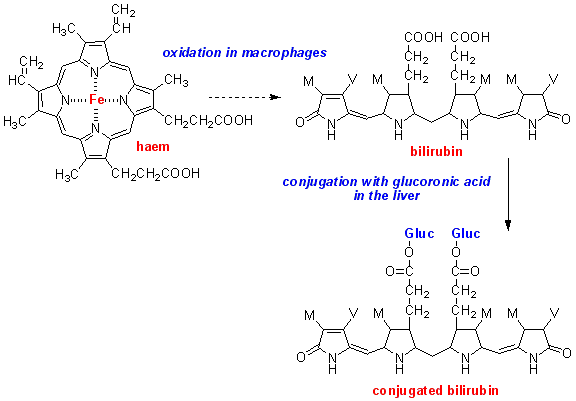
Jaundice is due to an abnormally high concentration of bilirubin, one of the bile pigments in the bloodstream.
Macrophages
take up old red blood cells and oxidise the haem of haemoglobin to bilirubin.
Bilirubin is then conjugated with glucuronic acid in the liver, and excreted
in the bile.
(A number of metabolites of drugs and other foreign compounds (xenobiotics), as well as physiological compounds such as steroid hormones, are conjugated with glucuronic acid in the liver and excreted in the bile.)
Conjugated bilirubin is one of the main compounds that colour faeces. If bilirubin is not excreted in the bile, the faeces will be pale coloured. The bilirubin accumulates in the bloodstream, giving the skin and whites of the eyes a yellow colour, and is excreted in the urine, giving it a dark colour.
What are the two main reasons why jaundice may occur?
Jaundice may occur as a result of:
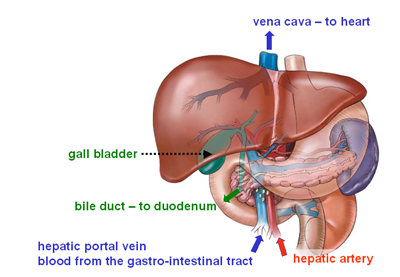
obstruction of the bile duct, so that bile cannot leave the gall bladder
liver disease (e.g. the various types of viral hepatitis, or alcoholic liver
disease)
How might you distinguish between these two causes of jaundice?
In liver disease the liver has a reduced capacity to conjugate bilirubin, so that there will be unconjugated bilirubin in the circulation.
In obstructive jaundice the liver can conjugate bilirubin normally, but there is impairment of its excretion in bile, so that there will be conjugated bilirubin in the circulation.
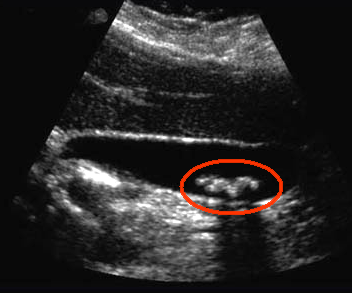 A
blood test showed that Ms GS had a high concentration of conjugated bilirubin
in her circulation, suggesting obstructive jaundice. She was sent for ultrasound
scan, which revealed the presence of gall stones, as shown on the right.
A
blood test showed that Ms GS had a high concentration of conjugated bilirubin
in her circulation, suggesting obstructive jaundice. She was sent for ultrasound
scan, which revealed the presence of gall stones, as shown on the right.
She then underwent cholecystectomy (surgical removal of the gall bladder); the excised gall bladder and the gall stones are shown below:

Chemical analysis of the gall stones showed that they were composed mainly of cholesterol, with a small amount of phospholipid and some calcium salts.
What are the main constituents of bile?
Apart from electrolytes, the main constituents of gall bladder bile are as follows (mmol /L):
| conjugated bilirubin | 5.1 |
| cholesterol | 16.0 |
| lecithin and other phospholipids | 3.9 |
| bile salts | 145.0 |
What are the bile salts, and how are they synthesised?
The bile salts are conjugates of cholic acid and chenodeoxycholic acid with glycine and taurine.
Normally the ratio of glycine : taurine conjugates is about 3 : 1.
They are synthesised in the liver by hydroxylation and side-chain oxidation of cholesterol, followed by conjugation with glycine or taurine.

What is the function of the bile salts?
The bile salts are amphiphilic molecules, with a hydrophobic planar hydrocarbon ring and a hydrophilic region provided by the hydroxyl groups and the glycine or taurine conjugated to the carboxylic acid group above the plane of the ring. In an aqueous medium the bile salts will form micelles on their own, and in bile they also emulsify the cholesterol that is secreted in the bile, so keeping it in solution. The phospholipids in bile also help to emulsify the cholesterol.
The function of the bile salts in the small intestine is to emulsify dietary lipids into mixed micelles that are small enough to be absorbed across the intestinal mucosa.
Cholesterol is extremely insoluble in water, and it needs only a relatively small increase in the content of cholesterol, or decrease in the concentration of bile salts, in the bile for it to crystallise, forming gall stones. In many cases gall stones are asymptomatic, since they are small enough to pass through the bile duct into the duodenum.
Why do you think Ms GS's faeces floated in the lavatory pan?
This is due to the presence of an excessive amount of unabsorbed triacylglycerol in her faeces. As a result of impaired absorption because of failure of bile secretion she was unable to form micelles small enough to be absorbed across the intestinal mucosa.
Why do you think Ms GS suffers from "gripping abdominal pain" after a meal?
 This is due
to transient obstruction of the bile duct as the gall bladder contracts to secrete
bile into the duodenum in response to stimulation by the presence of food in
the duodenum
This is due
to transient obstruction of the bile duct as the gall bladder contracts to secrete
bile into the duodenum in response to stimulation by the presence of food in
the duodenum
What is the function of the gall bladder?
Can Ms GS survive after cholecystectomy?
 The function
of the gall bladder is to concentrate and store bile until it is required for
secretion.
The function
of the gall bladder is to concentrate and store bile until it is required for
secretion.
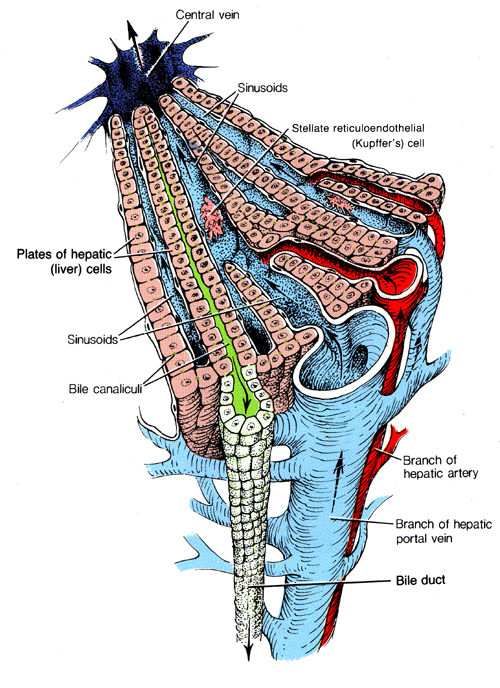
The compounds that will form bile are synthesised in hepatocytes and are secreted into the bile caniculi, shown in green in the diagram on the right. These drain into bile ducts that enter the gall bladder.
Not all mammals have a gall bladder - for example the rat does not, although mice do. This suggests that the gall bladder is not essential for lipid digestion and absorption, although bile itself is.
In the absence of a gall bladder, what will be secreted into the duodenum is hepatic bile, which is less concentrated than gall bladder bile:
| hepatic bile (mmol /L) | gall bladder bile (mmol /L) | |
| conjugated bilirubin | 0.7 |
5.1 |
| cholesterol | 2.6 |
16.0 |
| lecithin and other phospholipids | 0.5 |
3.9 |
| bile salts | 26.0 |
145.0 |
This means that without a gall bladder what will be secreted into the duodenum is a larger volume of more dilute bile. In the small intestine much water is reabsorbed anyway, so secretion of dilute bile will not lead to dehydration.
Average secretion of bile salt conjugates is of the order of 75 mmol per day, but only very small amounts are normally found in faeces.
What conclusions can you draw from this observation?
It seems likely that bile salts are reabsorbed from the small intestine and recycled. Interestingly, they are not absorbed from the micelles that contain monoacylglycerol, non-esterified fatty acids, phospholipids and cholesterol. Instead, as the other lipids are absorbed into intestinal epithelial cells from the micelles, the remnants for micelles that consist more or less completely of bile salt conjugates. These are absorbed in the terminal ileum.
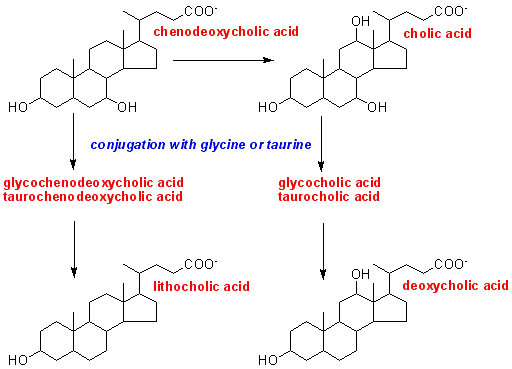 Analysis
of bile shows the presence of four bile acids, conjugated with glycine and taurine:
chenodeoxycholic and cholic acids, which are synthesised from cholesterol by
isolated hepatocytes, and deoxycholic acid, as well as a small amount of lithocholic
acid, neither of which is synthesised by isolated hepatocytes.
Analysis
of bile shows the presence of four bile acids, conjugated with glycine and taurine:
chenodeoxycholic and cholic acids, which are synthesised from cholesterol by
isolated hepatocytes, and deoxycholic acid, as well as a small amount of lithocholic
acid, neither of which is synthesised by isolated hepatocytes.
When the glycine and taurine conjugates of chenodeoxycholic acid and cholic acid were incubated with a mixed culture of faecal bacteria, free chenodeoxycholic acid and cholic acid were found in the incubation medium, together with two new compounds: lithocholic acid and deoxycholic acid.
What conclusion can you draw from this observation?
Intestinal bacteria seem to be able to deconjugate the conjugated bile acids, and metabolise them further, to lithocholic and deoxycholic acids.
The fact that these intestinal bacterial metabolites are secreted in bile is further evidence that the bile salts are reabsorbed from the small intestine, either before or after bacterial metabolism, and are recycled.
Although some 75 mmol of bile salts are secreted each day, the total body pool is only about 7.5 - 12.5 mmol; each molecule is secreted and reabsorbed some 6 - 10 time daily.
Chenodeoxycholic and cholic acid are generally referred to as primary bile salts, because they are synthesised in the liver; lithocholic and deoxycholic acids are referred to as secondary bile salts.
Gall stones in a young man
CD is a 20 year old man who went to see his GP because of persistent abdominal pain, diarrhoea and weight loss. On examination his abdomen was distended, and the pain was localised in the lower right of this abdomen. After a series of investigations he was found to have Crohn's disease affecting the terminal ileum. Treatment with steroids was ineffective in reducing the intestinal inflammation, and eventually he underwent surgery to remove the inflamed region.
Two years after the surgery he developed jaundice and complained of "gripping abdominal pain" after meals. An ultra-sound scan showed that he had a distended gall bladder and a number of gall stones.